 Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Krishna Prasad T*
Department of Anaesthesiology and Critical Care, Shri Sathya Sai Medical College and Research Institute, SBV Deemed University, Ammapettai, India
Correspondence to: Krishna Prasad T, Department of Anaesthesiology and Critical Care, Shri Sathya Sai Medical College and Research Institute, SBV Deemed
University, Ammapettai, India
Received date: May 25, 2022; Accepted date: June 06, 2022; Published date: June 13, 2022
Citation: Prasad TK (2022) Ease of Single Prick Popliteal Sciatic Block in a Modified Lateral Position. J Clin Anesthes Res 3(1): pp. 11-12. doi: 10.52916/jcar224011
Copyright: ©2022 Prasad TK. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Ultrasound, Anesthesia, Sciatic nerve, Local anaesthetics, Block
Ultrasound-Guided Popliteal Nerve Block has become a routine plan of anesthesia for below-knee Surgeries. It takes care of post-operative analgesia leading to the reduction of intravenous analgesia. In comparison to multiple pricks, single prick blocks are gaining importance since the success rate is the same, the duration of the procedure is less and patients cooperate better. Patients find to be in a prone position when compared to the lateral position and the ease of block is expected to be better in the lateral position. There are two approaches to block, commonest is the lateral approach which needs a change of needle direction and another prick to block both nerves.
There are two separate nerves tibial and common peroneal nerves. A perineural sheath envelops these two nerves from their origin in the pelvis, which is distinctly separate from the epineurium of each nerve. Giving local anesthesia within this sheath consistently gives a rapid onset and effective block, which is not considered to be an intraneural injection as long as the epineurium of individual nerves is not breached.
In the knee, just proximal to the popliteal fossa (50 and 120 mm proximal to the fossa), 7-8 cms above the popliteal creasethe sciatic nerve divides the tibial nerve along with collaterals supplies to calf muscles and the ankle joint. The perineal nerve supplies the knee joint and the area over the lateral aspect of the foot. In the fossa, the sciatic nerves are lateral and superficial to the artery and vein.
In the fossa, the sciatic nerves are lateral and superficial to the artery and vein. For the above reason, the lesser systemic toxicity is explained. Popliteal nerve block results in blocking the entire two third of the lower extremity, except the medial aspect of the leg, which is supplied by saphenous nerves, which cover only the superficial.
Depositing the local anesthetic where the nerves are separated yet in the common sheath (7-8 cms above the popliteal crease) further increases the pressure leading to patient discomfort, moreover, the muscles are closely placed which contributes to increased pressure inside the sheath. Hence, we would like to recommend the modified lateral approach patient in lateral position with the targeted limb above, which is only 2-4 cms above the popliteal fossa where both Trigeminal Neuralgia (TN) and Common Peroneal Nerve (CPN) already diverged into individual nerves, and away from Vloka’s sheath and also to observe the individual distribution of local anaesthetics in both the nerve sheath.
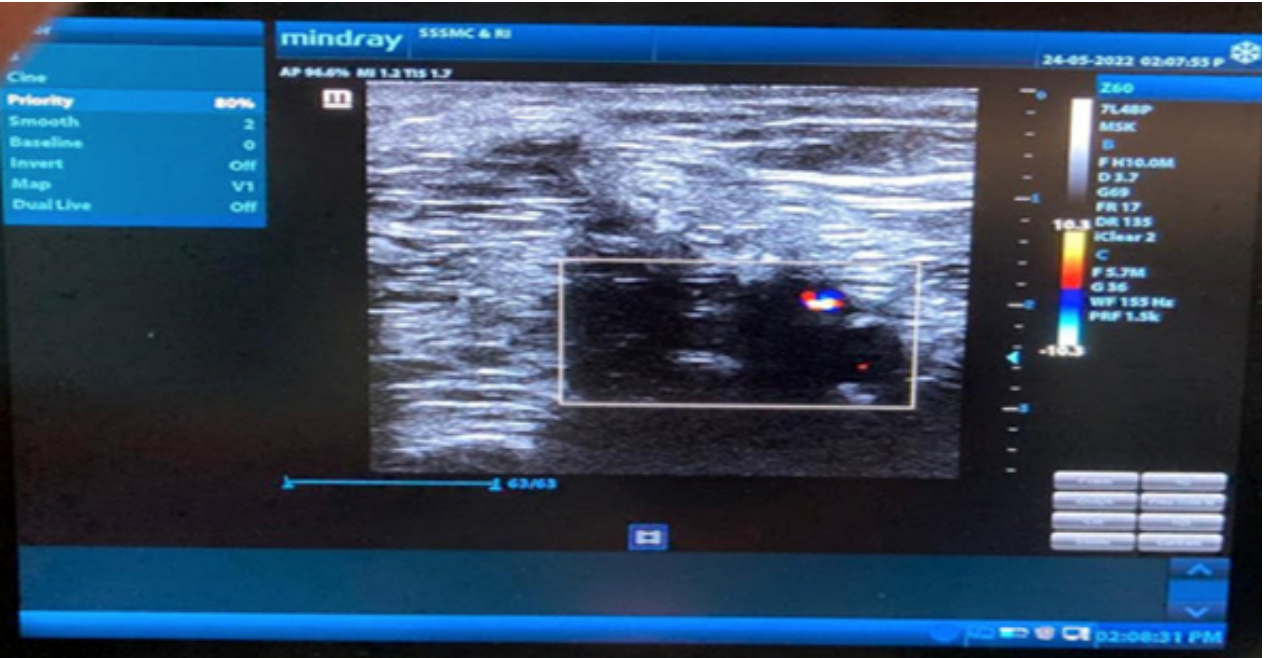 Figure 1: Sonoanatomy of the Sciatic Nerve at the popliteal fossa when the
patient is placed in lateral position. The divisions of the sciatic nerve i.e.
the Tibial Nerve (TN) and the Common Peroneal Nerve (CPN), is seen superficial and lateral to the Popliteal Artery (PA). This image was taken at
2 cm above the popliteal fossa where the TN and CPN have diverged into
individual nerves.
Figure 1: Sonoanatomy of the Sciatic Nerve at the popliteal fossa when the
patient is placed in lateral position. The divisions of the sciatic nerve i.e.
the Tibial Nerve (TN) and the Common Peroneal Nerve (CPN), is seen superficial and lateral to the Popliteal Artery (PA). This image was taken at
2 cm above the popliteal fossa where the TN and CPN have diverged into
individual nerves.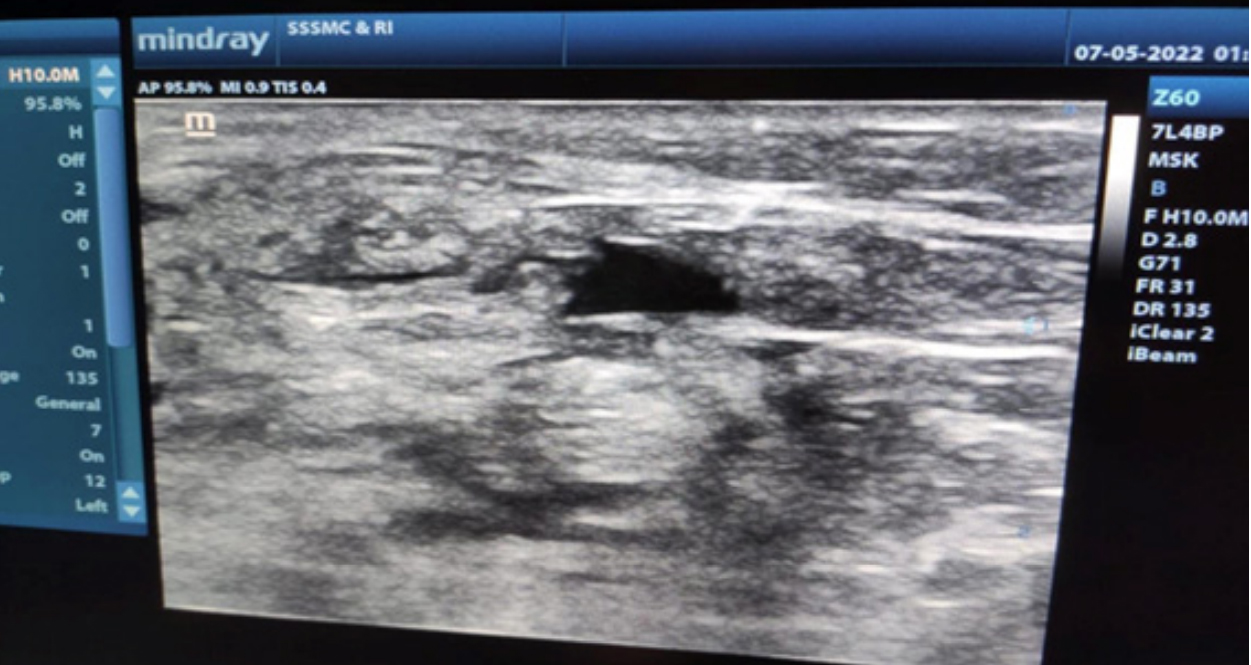 Figure 2: Sonoanatomy of the Sciatic Nerve at the popliteal fossa when the
patient is placed in lateral position shows needle path and local anaesthetic
distribution around individual nerves i.e. the sciatic nerve (TN and CPN) with
the ultrasound probe kept 2-3 cms away from the popliteal fossa.
Figure 2: Sonoanatomy of the Sciatic Nerve at the popliteal fossa when the
patient is placed in lateral position shows needle path and local anaesthetic
distribution around individual nerves i.e. the sciatic nerve (TN and CPN) with
the ultrasound probe kept 2-3 cms away from the popliteal fossa.Since the development of ultrasound technology has become a part of the perioperative period, ultrasound-guided nerve blocks have been largely used in the anesthesia and postoperative analgesia management of fracture surgery [1]. Moreover, when the patient is critically ill having sepsis, or cardiac issues, Peripheral Nerve Block (PNB) can be used as sole anaesthetic technique [2].
Putting the patient in the prone position and getting back to supine with severe injuries is not only time consuming but also can worsen the injuries and cause a lot of discomfort to the patient. Moreover, when the sciatic nerve is blocked in the prone position, patients will require their position to be changed for additional Femoral Nerve Block (FNB) and/or surgery making it more cumbersome.
Hence, we state that the approach to the sciatic nerve at the popliteal fossa in the modified lateral position under ultrasound guidance. It is easy to perform under ultrasound guidance and will require minimal position changes when compared to prone. Our approach in the lateral position will not require elevation of the patient’s lower limb making the patient more comfortable in comparison to the prone position. The limb was slightly flexed at the knee joint and hip.
Most commonly the sciatic nerve at the popliteal fossa is blocked by placing the tip of the needle within the common sciatic nerve sheath following which to the local anaesthetic is administered. This is appreciated by the distribution of local anaesthetic within the sheath and separation of the Tibial Nerve and Common Peroneal Nerve within Vloka’s sheath.
In a modified lateral position, we propose to deposit the local anaesthetic on the individual nerve through a single prick trying to deposit the local anaesthetic onto each nerve by placing the ultrasound probe 2-4 cms above the popliteal fossa where both TN and CPN already diverged into individual nerves, and away from Vloka’s sheath (Modified Lateral Position). Since, we aim to block the individual nerves, the time of onset is expected to be less when compared to the local anaesthetic being deposited within the sheath. We don’t expect a big difference in the duration of the block since this is going to be a single prick technique. In modified lateral technique, we would want to compare the duration of sensory and motor block and postoperative analgesia with the traditional technique i.e. when the local anaesthetic is deposited within the sciatic sheath by using the same local anaesthetics for both the groups. Further scope is to study in a group of patients as a comparative study with the other known approaches.
Respub Journals an online international open access organization which publishes all kinds of peer reviewed articles in the journals. Respub Journals focus into the fields of Clinical and Medical.

Attribution 4.0 International (CC BY 4.0). With this license readers can share, distribute, download, even commercially, as long as the original source is properly cited.
About ResPub
Responsibilities of Reviewers
Guidelines For Editors
Special Issue
Ethics And Policies
Payment
