 Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Parin Lalwani1, Chhavi Sawhney2*, Lokesh Kashyap2
1Assistant Professor, Department of Anaesthesiology Pain Medicine and Critical Care, All India Institute of Medical Sciences, New Delhi India
2Professor, Department of Anaesthesiology Pain Medicine and Critical Care, All India Institute of Medical Sciences, New Delhi India
Correspondence to: Chhavi Sawhney, Professor, Department of Anaesthesiology Pain Medicine and Critical Care, All India Institute of Medical Sciences, New Delhi
India.
Received date: December 4, 2020; Accepted date: December 15, 2020; Published date: December 22, 2020
Citation: Lalwani P, Sawhney C, Kashyap L (2020) Anaesthetic Challenges with DBS Device In Situ: Case Series with Review of Literature. J Clin Anesthes Res 1(1):
pp. 1-2. doi: 10.52916/jcar204004
Copyright: ©2020 Lalwani P, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Deep Brain Stimulation (DBS) can be an effective treatment option for patients with essential tremors, Parkinson’s disease, dystonia, epilepsy, chronic pain, major depression, and its role is being evaluated in a variety of other neurological diseases. Anesthesia concerns take into account the primary pathology for which the device was inserted, assessment of device functioning and its interference with diathermy, electrical electromagnetic, ultrasound, and laser devices used perioperatively for different purposes. We discuss anesthetic management with a brief review of two cases with DBS device In Situ.
Anesthesia, Parkinson’s disease, Deep Brain Stimulation (DBS), Bipolar cautery, Ultrasound.
Functional stereotactic neurosurgery, particularly Deep brain stimulation (DBS) is an effective treatment for Parkinson’s Disease (PD) and various movement disorders [1]. Anesthesiologists are likely to encounter patients with DBS devices more commonly as there are more than 1,50,000 patients with DBS all over the world [2]. These patients pose considerable challenges to the anesthesiologist because of advanced age, primary pathology and its complications, potential for interference with electromagnetic and monitoring devices. There is a paucity of literature describing anesthetic considerations for patients with DBS devices. We report anesthetic management of two patients with DBS devices.
A 55- year-old female patient was posted for debridement and implant removal of spino-pelvic fixation. She was a known case of PD with bilateral Subthalamic Nucleus (STN) DBS device (Medtronic Inc) in situ. Two years before she had a fall from height and developed spinopelvic dissociation along with bilateral distal femur and right calcaneal fracture. She had loss of consciousness for a few minutes but her NCCT head was normal. She underwent spinopelvic fixation, open reduction and internal fixation for fracture of femur and calcaneum under general anaesthesia (GA). All the surgeries were uneventful.
Now, the patient developed an infection at the implant site and was posted for debridement and spinopelvic implant removal. She was bedridden and her cardiovascular, respiratory, and airway examination was normal and she was not on any medication for PD. Neurological examination revealed cogwheel rigidity and pill-rolling movements of upper limbs. Besides routine investigations, a chest x-ray was done to see the implantable pulse generator (IPG) and its leads (Figure 1) which were found to be intact. Ultrasound-Guided (USG) doppler was done to rule out deep vein thrombosis and it was normal. In the preoperative period, information regarding the DBS model, current settings, battery status, and last check were obtained. On the morning of surgery tab syndopa 125 mg was given as advised by the neurologist.
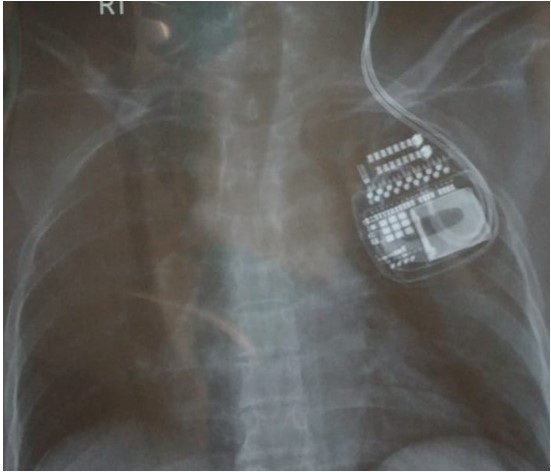 Figure 1: Chest X-ray showing an Implantable Pulse Generator (IPG) and its
leads.
Figure 1: Chest X-ray showing an Implantable Pulse Generator (IPG) and its
leads.Her baseline heart rate was 90 beats per minute (bpm) and BP was 130/90 mm Hg. Anesthesia was induced with propofol 50+20 mg, fentanyl 125 microgram, rocuronium 40 mg and the trachea was intubated. Rocuronium, N2O (50%) and isoflurane (0.6%-0.8%) in oxygen was used for maintenance. Monitoring included heart rate, non-invasive blood pressure, ECG, and pulse oximetry. DBS device was switched off after induction. The patient was turned lateral taking care to avoid neck stretching. All the pressure points including the DBS insertion site were padded. Bipolar cautery was used with a cautery plate placed under the buttock. The duration of surgery was 90 minutes.
At the end of the surgery, the DBS device was turned on and the original settings were restored. After the return of spontaneous respiration, neostigmine 2.5 mg and glycopyrrolate 0.4 mg was given and the trachea was extubated. The patient was conscious and haemodynamically stable
A 43-year old male with a solitary thyroid nodule was posted for hemithyroidectomy. He had a history of a head injury at the age of four years after which he developed spasmodic dystonia of the right side. DBS device was placed 19 years back. The battery was changed twice, 3 and 9 years after insertion.
Presently, the patient had mild movement disorder in the right upper limb. He was on tab trihexiphenidyl 2 mg tds and thyroxine 50 micrograms. Cardiac and respiratory system examination was within normal limits. X-ray soft tissue neck AP and lateral view (Figure 2) revealed extension wires connecting electrodes in the brain to IPG below the clavicle. DBS device was switched off a day before surgery after neurology consultation. In the operation theatre, routine monitoring was established. Anesthesia was induced with propofol, fentanyl and atracurium. The trachea was intubated with 8.0mm ID COETT. Anaesthesia was maintainedwith atracurium, fentanyl, air (50%), and isoflurane (0.8-1%) in oxygen. The head was placed in the neutral position rather than hyperextension of the neck with head elevation to prevent stretching or damage of the extension wires. Bipolar cautery was used and surgery lasted for two hours.
 Figure 1: X-ray neck showing DBS leads (Lateral and AP View).
Figure 1: X-ray neck showing DBS leads (Lateral and AP View).At the end of the surgery, the muscle relaxant was reversed and the trachea was extubated. The patient was conscious, haemodynamically stable and shifted to the recovery room with advice to switch on the DBS device after neurology consultation.
DBS system consists of one or more electrodes implanted within STN or globus pallidus interna which are tunneled subcutaneously via extension wires to IPG inserted subcutaneously below the clavicle or in the abdomen. These are programmed wirelessly with a handheld device.
Preoperative assessment of such patients should include interrogation of the device like indications for device insertion, battery lifespan and device functionality. The battery life is generally 2 to 5 years after which it is replaced.
Preoperative chest X-ray helps to identify the make and placement of the device and path of the wires [1]. It was more relevant in the second patient as the surgical field was close to the wires.
In the first case, a CT scan of the head, chest X-ray, and Doppler ultrasound was done for diagnostic purpose. In patient with a DBS device, plain X-ray, CT scan, fluoroscopy, and ultrasound can be performed safely with the transducer placed away from the device.
But the use of therapeutic ultrasound for phacoemulsification and harmonic scalpel generates heat and mechanical stress, thus it should be used with caution. Safety data on the use of MRI, laser, and extracorporeal wave lithotripsy is limited [2,3].
There is a potential for interference with electrical devices like electrocautery, short wave diathermy, peripheral nerve stimulators, defibrillators, and electroconvulsive therapy. We used bipolar cautery in both cases as the electrical current in bipolar mode is confined to tissue between the two electrodes of the electrosurgical unit.
In the intraoperative period, electrical signals generated by the device can lead to artifacts in electrocardiogram monitoring. Thus, it is advisable to switch off the device after induction of anesthesia as switching it off preoperatively may exacerbate neurological symptoms [4], as observed mild movement disorder in the second case.
In the first patient, single dose of levodopa was administered to prevent any exacerbation of neurological symptoms. Although the half-life of levodopa is 1-3 hours, the drug was not repeated as it was a short duration surgery.
In both cases, positioning was done carefully to avoid stretching or damage to the extension wires.
At the end of surgery switching on the device helps in proper arousal and may avoid recurrence of symptoms [5]. It is advisable to get the device examined for proper functioning in the postoperative period.
Perioperative management of brain pacemakers requires a multidisciplinary team including anesthesiologists, neurologists, surgeons, and DBS technicians. Interference of DBS with various electrical and electromagnetic devices may cause life-threatening complications this warrants strict alert and caution while using different monitoring, diagnostic and therapeutic modalities.
Respub Journals an online international open access organization which publishes all kinds of peer reviewed articles in the journals. Respub Journals focus into the fields of Clinical and Medical.

Attribution 4.0 International (CC BY 4.0). With this license readers can share, distribute, download, even commercially, as long as the original source is properly cited.
About ResPub
Responsibilities of Reviewers
Guidelines For Editors
Special Issue
Ethics And Policies
Payment
